

Monoclonal antibodies targeting CD38 are emerging as a mainstay of therapy for Multiple Myeloma (MM) in the relapse setting as well as upfront. These antibodies not only target CD38 on myeloma cells inducing anti-tumor pleiotropic effects, they also influence normal CD38‐expressing cells, including normal plasma cells, natural killer cells and immunosuppressive regulatory cells (van de Donk et al , 2018). These cells play a key role in innate as well as humoral immunity and provide protection against a variety of infectious insults; hence, their depletion in MM patients (pts) can be expected to have deleterious immunological effects due to the dismantling of an effective immune responses in a population already strained by dysfunctional immunity. While it has been previously shown that NK cells decline with exposure to daratumumab (DARA) (Casneuf et al , 2017), its clinical impact on the incidence of infection has yet to be elucidated because clinical trials have shown conflicting results, while POLLUX and CASTOR trials showed generally similar rates of grade 3 or 4 infections (28·3% vs. 22·8% and 21·4% vs. 19·0%, respectively, the ALCYONE trial, reported that grade 3-4 infections were higher in the DARA arm (23·1% vs. 14·7%). Here, we aim to explore the impact of different risk factors on infection during DARA therapy.
Methods: We retrospectively reviewed patient records who received DARA‐containing regimens for MM between Jan 2016 and Jan 2020. The history of infection, prior therapies, rate of infection during therapy with DARA, hospitalizations, baseline and nadir absolute counts of lymphocyte, monocyte and neutrophil population were extracted. Pts who had less than 1 month of DARA were excluded. Survival was measured from time of DARA start. Survival distribution was estimated using Kaplan-Meier methods and differences of OS, PFS between groups was examined by Wilcoxon test. The effect of treatment on OS and PFS was estimated using a Cox model after controlling for the effects of different variables.
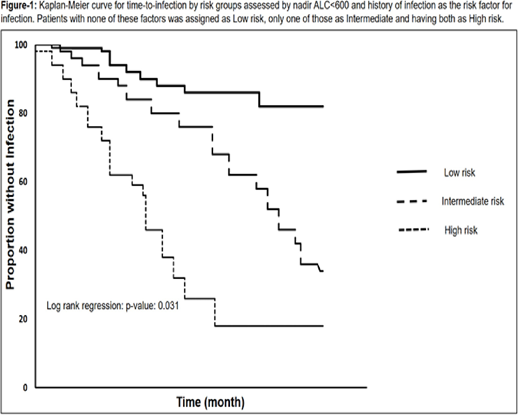
Results: Of 123 pts reviewed, median line of therapy was 3 (range: 0-9). Median time from diagnosis was 52 months (range: 0- 232 months). 43 pts (35%) were Black and 77 (63%) Caucasian. Median age was 70 (range 34-94 y/o). 86 (70%) were IgG, 24 were IgA (20%) and 10 light chain myeloma (10%). 24 (20%) had stage I, 37 (30%) had stage II and 61 (50%) had ISS stage III. 66 (53%) pts had transplant as prior therapy and the rest did not undergo transplant. 29 (24%) pts had DARA as a single agent, 66 (53%) in combination with IMiDs and 28 (23%) pts in combination with PI. Median duration of therapy was 133 days (range 30-1245 days). Median ANC 1243 /ml (range: 420-1120). Median ALC 710 /mL (170-8020). Median AMC was 455 /mL (0-2300). 31 pts had history of prior infections and the rest did not. 39 pts had infection during DARA. Overall, there were 125 hospital admission encounters for whole cohort occurred in 36% of cases, more than half of them (55%) were attributable to an infectious process. Bacterial pathogens accounted for the majority of infection. Pts with infection during DARA therapy had statistically significant nadir ALC (median 560 /ml) compared to pts without any infection. The univariate analysis showed age, history of infection, nadir ALC less than 600/ml and number of prior line of therapy as significant factors associated with infection rate during DARA therapy. Multivariate analysis after controlling for these factors shows only Low nadir ALC less than 600 /ml, hazard ratio (HR): 2.15, 95% confidence interval (CI): 1.19-3.76, and history of infection, HR: 1.87, 95% CI: 1.11-2.92, stands out as statistically significant factor. The whole cohort were divided based on ALC<600 during the therapy or history of previous infection; the group with none of these two risk factors was assigned as low risk, the group with either of those as intermediate risk and the pts with both risk factor were characterized as high-risk group (Figure-1).
Conclusion: Here we showed that infections is frequent among MM pts treated with DARA-containing regimen and assessed risk factors associated infection during DARA therapy. Dropping ALC and history of prior infection are significant factors associated with higher risk of infection during DARA therapy. These finding suggests vigilance for, and identification of risk factor are warranted for treating MM patient with DARA. The risk model is warranted to be examined in a prospective study.
de Lima:Pfizer: Other: Personal fees, advisory board, Research Funding; BMS: Other: Personal Fees, advisory board; Incyte: Other: Personal Fees, advisory board; Kadmon: Other: Personal Fees, Advisory board; Celgene: Research Funding. Malek:Cumberland: Research Funding; Takeda: Other: Advisory board , Speakers Bureau; Bluespark: Research Funding; Sanofi: Other: Advisory board; Clegene: Other: Advisory board , Speakers Bureau; Amgen: Honoraria; Medpacto: Research Funding; Janssen: Other: Advisory board, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal